
Hypertension is a cross gender issue. However, hypertension in women calls for concentrated focus if its considered the unique circumstances under which high blood pressure may occur among women.

Erroneously so, for a long time it was thought that women were at lower risk of hypertension related complications compared to men. We are referring here to complications such as heart attack, stroke and other cardiovascular diseases (CVDs).
This misconception may have generated less than necessary interest to provide more assertive attention to the effects of high blood pressure in women.
To the contrary, hypertension in women is a reality that exposes women to serious complications if left untreated seeing that pregnancy, menopause and the use of contraceptive pills, for example, are present triggers of hypertension in females. All these are special unique risk factors that women must contend with in the burdensome world of hypertension.
Being seized with the effect of hypertension in women should not be for physicians or researchers alone, but also women themselves hence our own efforts here in putting out to the surface issues involved when considering high blood pressure in women.

An eye opening 2012 review published in the journal, Therapeutic Advances in Chronic Disease (2012 May; 3(3): 137–146), shared an astonishing statistic indicating that two-thirds women with treated high blood pressure have uncontrolled hypertension.
In the meantime, a 2011 study carried out in Europe and published in the European Heart Journal (2011 Jun;32(11):1362-8) under the EuroHeart project, told a story that relative to men, the burden of cardiovascular disease is rising among middle-aged women. This rising burden also has its roots in a biased representation against women in scientific clinical trials, the report added.
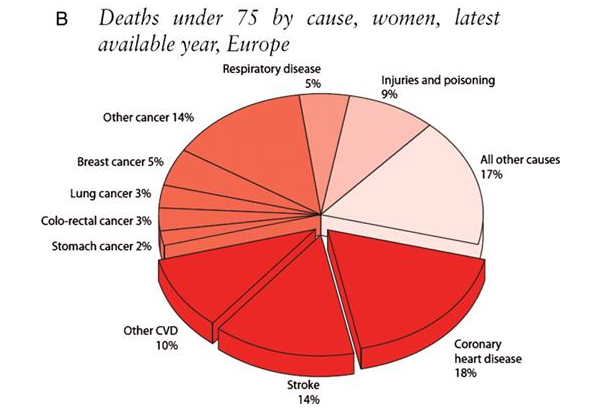
As mentioned, hypertension risks revolve around cardiovascular problems. We think the EuroHeart project beautifully highlighted the impact of hypertension in women through the following presentation.
Source: European Heart Journal
The shocking presentation you see above shows causes of death in Europe among women under the age of 75. Well known hypertension risks namely coronary heart disease, stroke and other CVDs constitute a combined 42% of the causes of death among women below the age of 75 in an advanced society!
Hypertension in women is major issue in industrialized societies so much that the misconception that cardiovascular disease is a man's problem is a problem in itself that calls for the "taking up of arms" in order to reduce hypertension related mortality and morbidity among women.
Be that as it may, given this kind of background there is value in considering in-turn specific triggers or circumstances under which hypertension in women uniquely occurs.

Menopause is a well known factor concerning high blood pressure in women. As such being a post-menopausal woman is a significant risk factor for hypertension.
A 1989 study shared in the Journal of Human Hypertension (1989 Dec;3(6):427-33) upheld this fact. It indicated that high blood pressure has a double prevalence in post-menopausal women compared to pre-menopausal women notwithstanding age and body mass index (BMI).
It was also shown in the study that sodium and potassium ratios change significantly post-menopause. We have written extensively about the link between potassium and high blood pressure as well as sodium and potassium ratios, a resource we highly recommend.
The 1989 study would not be the only study blaming post-menopause for hypertension in women. In 2000 another study published in the journal Maturitas (2000 Jan 15;34(1):25-32) equally pointed a finger at being post-menopausal as a risk factor for being hypertensive.
The 2000 Italian study involved over 22 000 women experiencing menopause. The study concluded that women in post-menopause were at higher risk of developing hypertension.
Apart from post-menopause, the study also confirmed that being overweight and being of low physical activity are also viable risks factors for high blood pressure in women during the post-menopause period.
If post-menopause is linked to hypertension in women, the questions becomes how does it do this. This question is essentially asking about what is known in biochemical science as the mechanism of action.
Hypertension researchers have postulated that sex hormones are behind the mechanism that leads to elevated blood pressure in post-menopausal women. It has been put forward that the drying up of endogenous estrogen which itself has been referred to as a sex-steroid hormone results in hypertension.
Researchers state that estrogen is a powerful vasolidator of which vasolidation refers to the widening of the blood vessels which is critical to blood pressure regulation.
The full chain of reasoning behind this proposed mechanism is as follows.
Post-menopausal women are at risk of hypertension because they have a reduced level of estrogen, for example, which in turn erodes their sysetm's ability to dilate blood vessels to allow unrestricted flow of blood in the blood vessels. This is what has been thought, at least in part, to cause elevated blood pressure in post-menopausal women
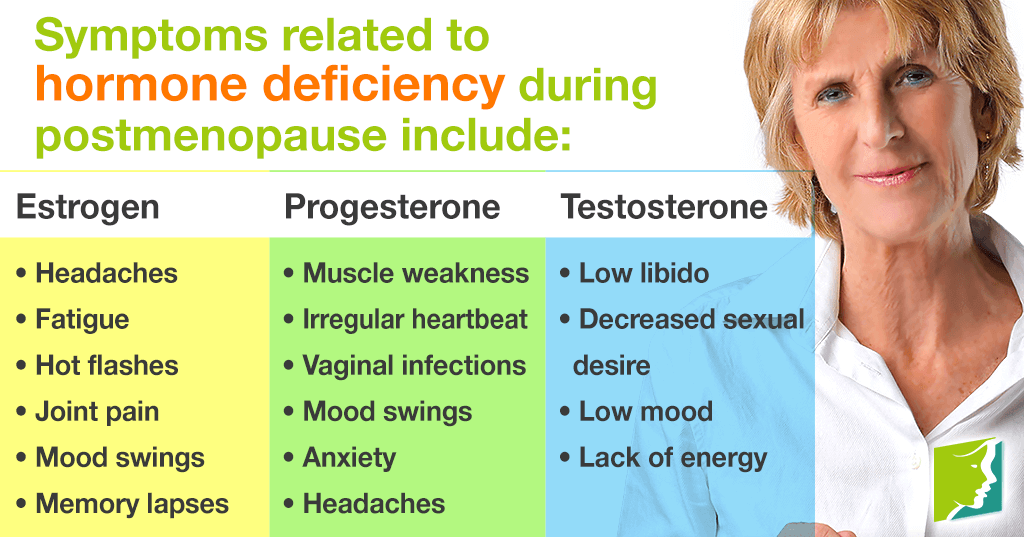
To top it off, below is an infographic illustrating the full range of hormones that are in decline during post-menopause and their related symptoms.
Source: 34 Menopause Symptoms
The use of contraceptives puts women at risk of hypertension. Also known in short as OCPs, combined estrogen and progestin oral contraceptive pills have been associated with elevated blood pressure in women as well as stroke, a cardiovascular event.
A 1981 review published in The Journal of Cardiovascular Medicine (1981 Apr;6(4):381, 384-7) shared that prolonged use of oral contraceptives increased blood pressure and acutely increased the risk of hypertension in women.
The report did not end there. It added that vulnerability to oral contraceptive induced hypertension in women was compounded by other important factors such as age, family history of high blood pressure, preexisting renal disease, not having given birth before and obesity.
Furthermore, the report stated that within half a year of using contraceptive pills, blood pressure would rise in a mild and uncomplicated fashion seldom requiring any medication. In the those women who are fortunate, elevated blood pressure due to oral contraceptive use could delay for as long as 6 years.
Despite these seemingly mild hypertension effects of pills in women, what was alarming in the report is that although small in number, some women were at risk of developing severe and sometimes life-threatening hypertension. The researchers pointed out that malignant hypertension and irreversible renal failure have occurred in some women following oral contraceptive pills.
What this points to, as hypertension scientists recommend, is that thorough medical checks must take place prior to the use of oral contraceptives. These would include physical examination with an eye on the cardiovascular system, repeated blood pressure measurements to also avoid white coat syndrome, urinalysis, blood urea and nitrogen and serum creatinine tests.
The Journal of Cardiovascular Medicine report strongly recommended that women who develop hypertension or who experience a high diastolic pressure of 90 mm Hg whilst taking the pills should stop immediately.
Be that as it may, the mechanism behind oral contraceptives and hypertension in women is not fully understood. It is, however, thought that contraceptive pills result in a combination of things namely arterial stiffness, renin–angiotensin system stimulation, and salt and water retention all of which are a poor concoction for normal blood pressure.
The unique situation that women vs men hold as it pertains hypertension is further illustrated by what happens to a worrying number of women when pregnant...
Between 6 and 10% of pregnant women suffer the complications of pregnancy induced hypertension. By definition gestational hypertension, as it is also known, is high blood pressure punctuated by a systolic blood pressure reading of greater than 140 mm Hg and a diastolic blood pressure reading of greater than 90 mm Hg.
Complications of pregnancy induced hypertension affect both mother and baby (born and unborn). Premature births and stillbirths are typical complications affecting the baby including later life hypertension and cognitive problems. The mother itself will also suffer possible progression of what begins as pregnancy hypertension to essential hypertension with higher risks of cardiovascular diseases.
We have already devoted a great deal of focus on pregnancy induced blood pressure and all its accompanying complications which you can see in detail here.
With all these considerations in respect of hypertension in women, perhaps the natural question that follows is treatment of high blood pressure in women.
Studies have shown that women have a greater overall contact with physicians than men and therefore have greater awareness of their hypertension status than men.
In this regard, the 1999-2004 National Health and Nutrition Examination Survey (NHANES) report in the United States showed that 68% of hypertensive women were knowledgeable of their status compared to 67% of hypertensive men. This trend followed in treatment were 58% of hypertensive women vs 52% of hypertensive men were under any antihypertensive treatment.
Below we list possible treatment options of hypertension in women informed by circumstances inducing the high blood pressure in the first place.
In cases were pills are causing high blood pressure, discontinuation is often the most effective method of treating oral contraceptive-induced hypertension.
However, as noted earlier in yet some other cases depending on the length of time the pills were used and the damage caused the damage itself my result in secondary hypertension even when taking pills is stopped.
Some researchers have also stated that women suffering estrogen-induced hypertension, could also try oral contraceptives containing only progestogen vs , for example, those containing both estrogen and progestogen.
It's been said the best treatment for gestational high blood pressure is delivery. While so simple, this is medically true. Depending on gestational age of the pregnancy, in some cases doctors are forced to initiate delivery of the pregnancy.
Bedrest has been identified in some studies as a very effective method of reducing and controlling high blood pressure in pregnancy. While sodium intake has been the rule of thump in general hypertension, this is surprisingly not the case in pregnant women. It is not regular practice that pregnant women should reduce their salt intake. Apparently, water retention effects of salt is beneficial in pregnancy due to declining blood vessel volume issues.
We have also covered in detail treatment options of high blood pressure in pregnancy in our gestational hypertension article.
While at first glance treatment of hypertension in men and women is not materially different, an in-depth consideration reveals some differentiating aspects.
This is to say not all pharmaceutical drugs used in men are suitable for women. For example, Angiotensin-converting enzyme (ACEs) and Angiotensin II receptor blockers (ARBs) are not to be used by pregnant women or women planning to fall pregnant due to their risk of baby development abnormalities.
What this tells us is that anti-hypertensive drugs are gender dependent such that while men are prone to developing gout upon using diuretics, women are at risk of developing abnormally low sodium (hyponatremia) or low levels of potassium in the blood (hypokalemia).
Furthermore, the 1993 Treatment Of Mild Hypertension Study (TOMHS) (1993 Aug 11;270(6):713-24) involving nearly 1000 women and men observed that women reported a two-fold rise in side effects than men.

Another 2004 study published in the journal Blood Pressure (2004;13(5):272-8) noted that on using ACE inhibitors, women developed coughing as a side effect 3 times more often than their male counterparts.
In addition, women also had a greater chance to complain of edema (fluid swelling) and hirsutism, a male-pattern hair growth, on using Combination Calcium Channel Blocker or CCBs. CCBs are are drugs used to treat hypertension or angina (chest pain or discomfort).
Finally, in both women men, sexual dysfunction is a common problem associated with treating hypertension using pharmaceutical drugs. In particular, beta-blockers and thiazide diuretics are known to bear these side effects.
[Last updated: 02 November 2017]

|
|
Alcohol and Blood Pressure |
Return to What Causes High Blood Pressure from Hypertension In Women
Return to High Blood Pressure Home from Hypertension In Women
Disclaimer
Information contained on this website is not meant to replace your doctor's advice.
(c) All Rights Reserved. 2010-2018
Jan 30, 18 03:06 PM

Jan 08, 18 05:25 AM

Jan 04, 18 01:52 PM















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}